What is your sex?
What is your sex?
Male
Female
*This question refers to your biological sex and not your gender identity. In general, the response that will generate the most accurate results is the sex that you were assigned at birth. If you are unsure of your response, remember that you can always repeat the assessment using an alternate response.
What is your height?
What is your height?
(Feet)
4
5
6
(Inches)
0
0.5
1
1.5
2
2.5
3
3.5
4
4.5
5
5.5
6
6.5
7
7.5
8
8.5
9
9.5
10
10.5
11
11.5
What is your date of birth?
What is your zip code?
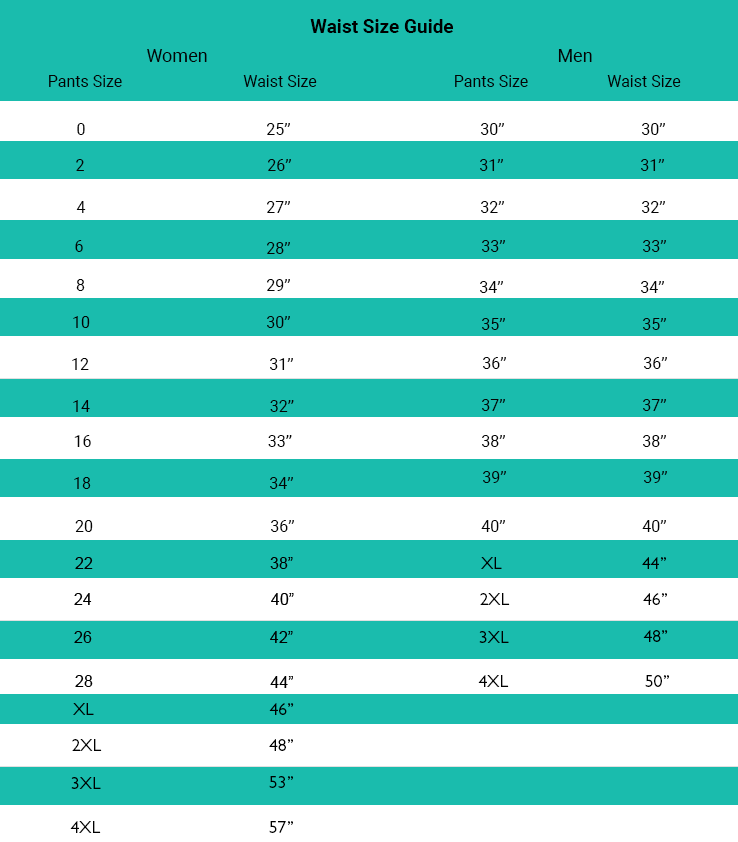
Waist Circumference (Inches)
Don’t know your waist size?Refer to the guide below or use a tape measure.
If measuring waist, center tape over belly button.
Current Weight (Pounds)
Highest Adult (Non-Pregnancy) Weight (Pounds)
What is your level of muscularity?
What is your level of muscularity?
Very High
High
Average
Low
In your own words, describe in one sentence your deepest and most meaningful reason for wanting to work on your fitness and weight now (your “Why”).
Is this your truest “Why” or is there a deeper reason?
Is this your truest “Why” or is there a deeper reason?
No, let me try again
Yes, I’m happy with this reason
Why are you interested in taking action NOW to address your fitness and/or nutrition? Select one
Why are you interested in taking action NOW to address your fitness and/or nutrition? Select one
Upcoming event
Health professional recommendation
Recent weight gain
Recent inactivity
Recent stress level
Recent sleep issues
Recent health issue
Recent relocation
Recent injury
Looking for new approach
Referral from friend
Other
Please characterize your participation in consistent, planned exercise across the past year on average.
Please characterize your participation in consistent, planned exercise across the past year on average.
Exercise less than 3 days per week for 30 minutes or more
Light exercise 3 or more days per week for 30 minutes or more
Moderate exercise 3 or more days per week for 30 minutes of more
Intense exercise 3-5 days per week for 30 minutes or more
Intense exercise 6-7 days per week for 30 minutes or more
Please select the response that best characterizes your weight goal.
Please select the response that best characterizes your weight goal.
Maintain current level of body fat
Lose 1-10 pounds of body fat
Lose 11-20 pounds of body fat
Lose 21-30 pounds of body fat
Lose 31-40 pounds of body fat
Lose 41-50 pounds of body fat
Lose 51-75 pounds of body fat
Lose 76-100 pounds of body fat
Lose over 100 pounds of body fat
Please select the response that best characterizes your fitness goal.
Please select the response that best characterizes your fitness goal.
Maintain current level of fitness
Small improvement in level of fitness
Moderate improvement in level of fitness
Large improvement in level of fitness
Very large improvement in level of fitness
On a scale of 0 to 5, with 5 being most important and 0 being least important, please indicate the level of importance of each item below to your desire to improve your fitness and weight.
On a scale of 0 to 5, with 5 being most important and 0 being least important, please indicate the level of importance of each item below to your desire to improve your fitness and weight.
Health & Wellness
Appearance & Self-Esteem
Social Engagement
Performance
On a scale of 0 to 5, with 5 being most challenging and 0 being least challenging, please score the level of challenge that you face from each item below in achieving your fitness and weight goals.
On a scale of 0 to 5, with 5 being most challenging and 0 being least challenging, please score the level of challenge that you face from each item below in achieving your fitness and weight goals.
Time & Schedule
Motivation & Support
Goal-Setting & Structure
Fitness & Nutrition Knowledge
On a scale of 0-5, with 0 being lowest and 5 being highest, how would you characterize your level of unhealthy stress in the following settings:
On a scale of 0-5, with 0 being lowest and 5 being highest, how would you characterize your level of unhealthy stress in the following settings:
Work or School: (drop down response 0-5)
Home: (drop down response 0-5)
Social Engagements: (drop down response 0-5)
Recent/Chronic Injuries and Medical Events
Recent/Chronic Injuries and Medical Events
Back Injury
Sciatica
Knee Injury
Hip Injury
Elbow Injury
Wrist Injury
Ankle Injury
Fracture
Dislocation
Shin Splints
Bursitis
Muscle or Ligament Tear
Recent Surgery
Delivery/Pregnancy
Shoulder Injury
Other (Click to enter)
NONE
Scroll Through List And Select ALL Diagnosed Conditions That Apply To You.
Scroll Through List And Select ALL Diagnosed Conditions That Apply To You.
High Blood Pressure
High Cholesterol
High Triglycerides
Acid Reflux/Heartburn/Indigestion
Back Pain
Joint Pain
Fatigue/Low Energy
Shortness of Breath Under Exertion
Irritable/Irregular Bowel
Adult Acne
Frequent Headaches
Frequent Muscle Aches
Muscle Twitching or Cramps
Frequent or Lengthy Colds
Constant Feelings of Stress or Anxiety
Frequent Sugar Cravings
Daytime Drowsiness
Brain Fog/Poor Concentraion
Frequent or Easy Bruising
Depression
High Blood Sugar/Prediabetes
PCOS
Hyperuricemia
Irregular Cycle/Infertility
Sleep Apnea
Poor Circulation
Restricted or Limited Mobility
Edema/Swelling
Slow Healing
Uncontrolled Eating/Food Addiction
Non-Age Memory Loss
Non-Age Cognitive Decline
Jaundice (yellowed skin)
Low Kidney Function (including Dialysis)
Type 2 Diabetes
Fatty Liver
Heart Disease
Gout
Gallstones
Osteoarthritis
Neuropathy
Gangrene and/or Amputation
Early Onset Alzheimers
History of Stroke
History of Endometrial Cancer
History of Esophogeal Cancer
History of Gastric Cancer
History of Liver Cancer
History of Kidney Cancer
History of Pancreatic Cancer
History of Colorectal Cancer
History of Meningioma (Brain Cancer)
History of Multiple Myeloma (Blood Cancer)
History of Gall Bladder Cancer
History of Ovarian Cancer
History of Post-Menopausal Breast Cancer
History of Throid Cancer
NONE
How many commercial diet plans have you followed (for at least 30 days) in the last five (5) years?
How many commercial diet plans have you followed (for at least 30 days) in the last five (5) years?
20+ diet plans followed
15-19 diet plans followed
10-14 diet plans followed
6-9 diet plans followed
3-5 diet plans followed
1-2 diet plans followed
0 diet plans followed
Your current level of overall fitness for your age is:
Your current level of overall fitness for your age is:
Very Low
Low
Moderate
High
Very High
What supplementation do you take regularly? (check all that apply)
What supplementation do you take regularly? (check all that apply)
I do not take supplements
Multivitamin
Apple Cider Vinegar
Ashwagandha
BCAAs
Borage
Calcium
CBD
Chondroitin
Chromium
Cinnamon
Coconut Oil
Collagen
CoQ10
Creatine
Curcumin/Tumeric
Digestive Enzymes
Fish Oil/Krill Oil/Algae Oil/Omega-3
Flaxseed
Folic Acid
Gingko
Ginseng
Glucosamine
Green Tea Extract
Iron
L-Arginine
L-Carnitine
Magnesium
Manganese
Melatonin
Milk Thistle
Niacin
Potassium
Pre-Workout
Probiotics
Protein Powder
Resveratrol
Selenium
St. John’s Wart
Taurine
Tyrosine
Valerian
Vitamin B Complex
Vitamin B12
Vitamin C
Vitamin D
Vitamin E
Vitamin K
Zinc
Other
What fitness activities have you enjoyed (in the past?)?” (check all that apply)
What fitness activities have you enjoyed (in the past?)?” (check all that apply)
Aerobics
Barre
Basketball
Body Weight Exercise/Calisthenics
Bootcamp
Boxing
Circuit Training
Dance
Golf
Gymnastics
HIIT
Hiking
Indoor Cycling
Jogging or Running
Jumping Rope
Kickboxing
Martial Arts
Outdoor Cycling
Pilates
Racquetball
Rock Climbing
Rowing
Skiing
Soccer
Squash
Stair climber
Step Aerobics
Stretching
Swimming
Tai Chi
Tennis
Volleyball
Walking
Water Aerobics
Weight Lifting
Yoga
Other
When do you prefer to workout? Select all that apply
When do you prefer to workout? Select all that apply
Monday
Morning
Afternoon
Evening
Tuesday
Morning
Afternoon
Evening
Wednesday
Morning
Afternoon
Evening
Thursday
Morning
Afternoon
Evening
Friday
Morning
Afternoon
Evening
Saturday
Morning
Afternoon
Evening
Sunday
Morning
Afternoon
Evening
How often to you smoke tobacco or use a vaporizer?
How often to you smoke tobacco or use a vaporizer?
Daily
Occasionally
Never
Which of the following recovery practices do you engage in on a consistent basis following exercise?
Which of the following recovery practices do you engage in on a consistent basis following exercise?
Foam Rollers
Percussive Therapy Guns
Heat Therapy (Such as Steam and Sauna)
Light Therapy (Such as Infrared and Red Light)
Cold Therapy (Such as Cryotherapy or Cold Packs)
Compression Therapy
Hyperbaric Therapy or Floatation Therapy
None
First Name
Last Name
Email
Mobile Number
State
Select
California
Country
Select
United States
United States Minor Outlying Islands
Afghanistan
Albania
Algeria
American Samoa
Andorra
Angola
Anguilla
Antarctica
Antigua and Barbuda
Argentina
Armenia
Aruba
Australia
Austria
Azerbaijan
Bahamas
Bahrain
Bangladesh
Barbados
Belarus
Belgium
Belize
Benin
Bermuda
Bhutan
Bolivia
Bosnia and Herzegovina
Botswana
Bouvet Island
Brazil
British Indian Ocean Territory
Brunei Darussalam
Bulgaria
Burkina Faso
Burundi
Cambodia
Cameroon
Canada
Cape Verde
Cayman Islands
Central African Republic
Chad
Chile
China
Christmas Island
Cocos (Keeling) Islands
Colombia
Comoros
Congo
Congo, the Democratic Republic of the
Cook Islands
Costa Rica
Cote D'Ivoire
Croatia
Cuba
Cyprus
Czech Republic
Denmark
Djibouti
Dominica
Dominican Republic
Ecuador
Egypt
El Salvador
Equatorial Guinea
Eritrea
Estonia
Ethiopia
Falkland Islands (Malvinas)
Faroe Islands
Fiji
Finland
France
French Guiana
French Polynesia
French Southern Territories
Gabon
Gambia
Georgia
Germany
Ghana
Gibraltar
Greece
Greenland
Grenada
Guadeloupe
Guam
Guatemala
Guinea
Guinea-Bissau
Guyana
Haiti
Heard Island and Mcdonald Islands
Holy See (Vatican City State)
Honduras
Hong Kong
Hungary
Iceland
India
Indonesia
Iran, Islamic Republic of
Iraq
Ireland
Israel
Italy
Jamaica
Japan
Jordan
Kazakhstan
Kenya
Kiribati
Korea, Democratic People's Republic of
Korea, Republic of
Kuwait
Kyrgyzstan
Lao People's Democratic Republic
Latvia
Lebanon
Lesotho
Liberia
Libyan Arab Jamahiriya
Liechtenstein
Lithuania
Luxembourg
Macao
Macedonia, the Former Yugoslav Republic of
Madagascar
Malawi
Malaysia
Maldives
Mali
Malta
Marshall Islands
Martinique
Mauritania
Mauritius
Mayotte
Mexico
Micronesia, Federated States of
Moldova, Republic of
Monaco
Mongolia
Montserrat
Morocco
Mozambique
Myanmar
Namibia
Nauru
Nepal
Netherlands
Netherlands Antilles
New Caledonia
New Zealand
Nicaragua
Niger
Nigeria
Niue
Norfolk Island
Northern Mariana Islands
Norway
Oman
Pakistan
Palau
Palestinian Territory, Occupied
Panama
Papua New Guinea
Paraguay
Peru
Philippines
Pitcairn
Poland
Portugal
Puerto Rico
Qatar
Reunion
Romania
Russian Federation
Rwanda
Saint Helena
Saint Kitts and Nevis
Saint Lucia
Saint Pierre and Miquelon
Saint Vincent and the Grenadines
Samoa
San Marino
Sao Tome and Principe
Saudi Arabia
Senegal
Serbia and Montenegro
Seychelles
Sierra Leone
Singapore
Slovakia
Slovenia
Solomon Islands
Somalia
South Africa
South Georgia and the South Sandwich Islands
Spain
Sri Lanka
Sudan
Suriname
Svalbard and Jan Mayen
Swaziland
Sweden
Switzerland
Syrian Arab Republic
Taiwan, Province of China
Tajikistan
Tanzania, United Republic of
Thailand
Timor-Leste
Togo
Tokelau
Tonga
Trinidad and Tobago
Tunisia
Turkey
Turkmenistan
Turks and Caicos Islands
Tuvalu
Uganda
Ukraine
United Arab Emirates
United Kingdom
Uruguay
Uzbekistan
Vanuatu
Venezuela
Viet Nam
Virgin Islands, British
Virgin Islands, U.s.
Wallis and Futuna
Western Sahara
Yemen
Zambia
Zimbabwe
City
Select
Los Angeles
Location
Select
bodqr West
Create Password
Confirm Password
Back
Back
Next
Waist Size Guide
X
This email address is already registered.
Please log in to continue and view your results.
Email address
Password
Forgot Password?
Submit